Anterior Knee Pain | Patellofemoral Pain Relief
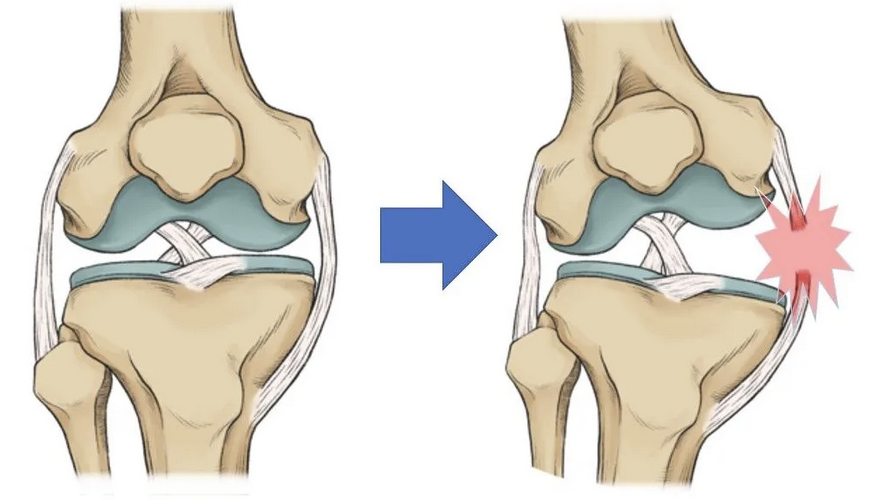
Patellofemoral Joint (PFJ) pain—one of the most common sources of anterior knee pain—typically presents as discomfort at the front of the knee, underneath the kneecap, or around the patella. With an accurate diagnosis and an individualised treatment plan we can help you return to the activities you love—stronger, more confident and pain-free.